

Vitamin B12 is one of the most important nutrients for energy, brain health, red blood cell production, and overall wellness. Yet not all forms of B12 are created equal, and knowing the difference can help you and your provider choose the best option for your needs. At Nervana Medical in Sandy, Utah, we specialize in functional and regenerative medicine, offering injectable and IV therapies tailored to optimize your health. In this guide, we break down the four main types of B12;methylcobalamin, hydroxocobalamin, adenosylcobalamin, and cyanocobalamin; highlighting how they work, which ones we stock in our clinic, and why certain forms are more effective for patients with fatigue, neurological issues, or genetic variants like MTHFR.
Quick Summary
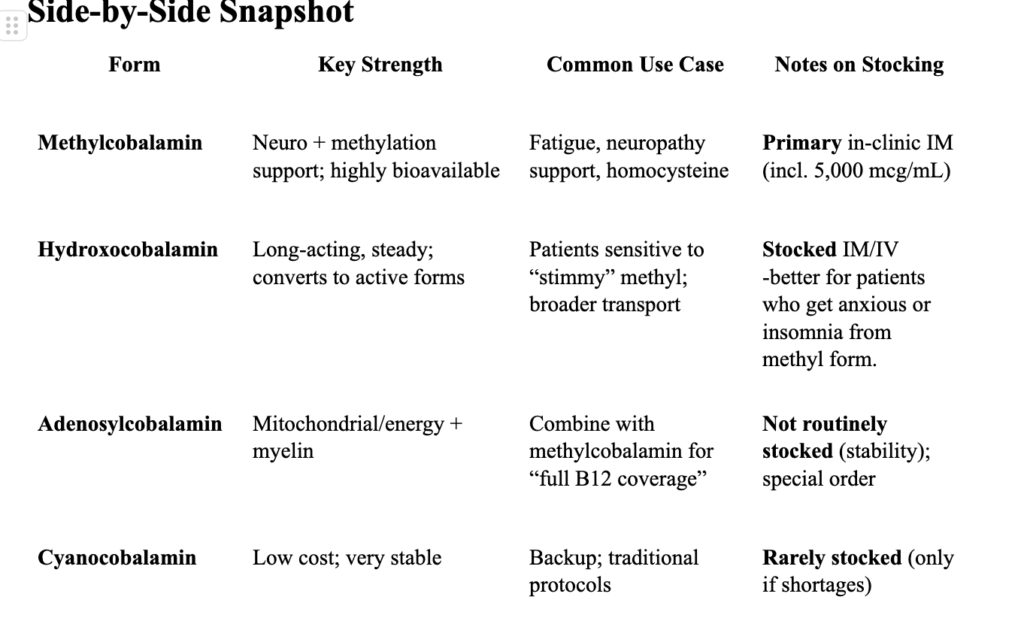
- Methylcobalamin – Active, methylated form. Neuro + methylation support.
- Primary form we stock (often 5,000 mcg/mL for IM use).
- Hydroxocobalamin – Naturally occurring, long-acting transport form; converts to methyl- and adenosylcobalamin as needed.
- We stock this; often preferred for patients who feel “wired” on high-dose methylcobalamin.
- Adenosylcobalamin – Active mitochondrial form (energy/Krebs cycle).
- We don’t routinely stock due to solution stability; may be special-ordered via compounding pharmacy.
- Cyanocobalamin – Stable, synthetic precursor that the body converts to active forms.
- We rarely stock (backup only). This is not an absorbable form for patients with the MTHFR gene mutation.
1) Methylcobalamin (MeCbl)
What it does: Active, methylated B12 used in homocysteine regulation, neurotransmitter synthesis, and nerve health.
Why we like it: Highly bioavailable; strong clinical track record for energy and neurologic support. Often best-tolerated for ongoing maintenance.
MTHFR: Excellent choice for patients with MTHFR variants (pairs well with L-methylfolate).
We stock: Yes; including concentrated 5,000 mcg/mL for IM.
2) Hydroxocobalamin (OHCbl)
What it does: A natural B12 form with a longer circulation time; the body converts it to methyl- and adenosylcobalamin.
Why we like it: Smooth, long-acting profile; often preferred when patients feel anxious or have insomnia with higher-dose methylcobalamin.
MTHFR: Fully usable even with MTHFR variants (MTHFR affects folate metabolism, not B12 absorption).
We stock: Yes (IM/IV per provider judgment).
3) Adenosylcobalamin (AdoCbl; “Dibencozide”)
What it does: The mitochondrial coenzyme form; supports cellular energy production and myelin integrity (works synergistically with methylcobalamin).
Why we don’t routinely stock it: Less chemically stable in solution (light/heat/oxygen sensitive) → shorter beyond-use dates and higher waste. Many pharmacies and IV clinics therefore prioritize methyl- and hydroxocobalamin.
How to access: Typically special-ordered via 503A compounding; commonly used orally or sublingually in combo with methylcobalamin.
4) Cyanocobalamin (CyanoCbl)
What it does: A very stable, synthetic B12 that the body converts to methyl- and adenosylcobalamin.
Pros/cons: Inexpensive and widely available; often requires more frequent dosing for maintenance. Contains a tightly bound cyanide group in trace amounts; clinically safe at therapeutic doses.
We stock: Rarely (used only during supply constraints of preferred forms). MTHFR gene mutation will not be able to break this form down. *This is the form of B12 in some formulations such as MICC, stay tuned for MICC 101 in a near future blog !
Safety, Interactions, and Precautions (high-level)
- Allergy/hypersensitivity: Avoid if known allergy to B12 or cobalt.
- Severe megaloblastic anemia repletion: Monitor potassium (rare hypokalemia when erythropoiesis resumes).
- Polycythemia vera: B12 replacement may “unmask” an underlying PV; monitor hematology.
- Drug factors that lower B12 absorption: Metformin, PPIs, H2 blockers, colchicine, some chemo agents; alcohol misuse.
- Special populations: In Leber hereditary optic neuropathy, caution with cyanocobalamin (rare optic issues noted historically).
- Renal/liver considerations: Dose/interval may need adjustment with significant organ disease; interpret very high serum B12 cautiously (could be a disease marker).
- In supplementation: High levels in healthy kidneys/liver are usually harmless; the body excretes excess.
- In organ disease: Elevated B12 should not be dismissed. It may indicate altered clearance, leakage from storage, or malignancy.
B12 Serum Levels
-If a patient has adequate B12 levels but still feel fatigue, we recommend interpreting serum B12 with MMA (methylmalonic acid) +/- homocysteine, which better reflects functional B12 status.
1. Methylmalonic Acid (MMA)
- Pathway: MMA rises when there’s not enough B12 to convert methylmalonyl-CoA → succinyl-CoA (mitochondrial pathway).
- Marker of: B12 deficiency only.
- Key point: If MMA is elevated, it’s almost always a sign of B12 deficiency (unless renal function is poor).
2. Homocysteine
- Pathway: Homocysteine → methionine requires both B12 and folate (and B6 indirectly in a different pathway).
- Marker of: Elevated in B12 deficiency, folate deficiency, and sometimes B6 deficiency.
- Key point: Homocysteine is sensitive but not specific; it will go up in multiple vitamin deficiencies.
Why this matters clinically: High homocysteine is a red flag that something in this network is off. Elevated homocysteine is linked to cardiovascular risk, cognitive decline, and clotting disorders.
Possible causes:
- Folate deficiency (no methyl group to donate).
- B6 deficiency (transsulfuration blocked).
- MTHFR mutation (can’t generate 5-MTHF efficiently → less methyl donor available).
- B12 deficiency (can’t transfer methyl group).
Key Points:
- B12 deficiency: ↑ MMA and ↑ homocysteine
- Folate deficiency: Normal MMA, ↑ homocysteine
- B6 deficiency (rare cause): Normal MMA, ↑ homocysteine
Renal disease: ↑ MMA (due to poor clearance), homocysteine may or may not be elevated - Pro tip* in iron deficiency anemia, the hallmark finding on a CBC and peripheral smear is microcytic, hypochromic red blood cells.
*We will cover different types of anemia in our next blog and how to interpret red blood cells, their size and their color! For more information on iron deficiency anemia in particular read here: https://www.nervanamedical.com/everything-you-need-to-know-about-venofer-and-iron-infusions/
4. Clinical use
- If serum B12 is low (<200 pg/mL) → deficiency is likely, but confirm with MMA ± homocysteine.
- If serum B12 is “borderline” (200–400 pg/mL) → order MMA ± homocysteine to assess functional status.
- If both are normal → unlikely to be clinically deficient.
- Optimal Levels that we typically shoot for are 1000-1200 pg/ml, this is where people will typically feel the benefits of improvement in fatigue
- Typical dose: 1,000–5,000 mcg daily or every few days (depending on serum levels and symptoms). Pro tip: High doses often preferred for neurological and energy-related benefits.
Why we push for higher “Optimal” Levels
- Safety: Vitamin B12 is water-soluble. In people supplementing with oral/IM/IV B12, serum levels of 1,000–1,100 pg/mL aren’t known to be harmful. Many wellness/IV clinics routinely see post-dose levels in this range (and higher) without toxicity.
- When to be cautious: Persistently high B12 without supplementation can be a disease marker (liver disease, renal impairment, myeloproliferative/solid tumors). If a patient isn’t taking B12 but runs >1,000–1,500 pg/mL, work up rather than celebrate.
Other Serum Lab Markers for B12:
- MMA (methylmalonic acid): normal/low = good cellular B12 status.
- Homocysteine: should normalize with adequate B12 (and folate/B6).
CBC/retic if correcting anemia; K⁺ early in severe megaloblastic anemia.
Who to adjust/space dosing for: significant CKD (slower clearance) or active liver disease (abnormal storage/release can skew serum B12). In these cases, consider longer intervals between injections and lean on MMA/homocysteine rather than the raw serum level.
- MMA = specific for B12
- Homocysteine = sensitive but not specific (B12, folate, or B6)
- Both elevated = B12 deficiency confirmed
- Only homocysteine elevated = more likely folate (or B6) deficiency
Best Forms for MTHFR Variants
- Top choices: Methylcobalamin (directly active) and Hydroxocobalamin (converts as needed; often better tolerated if “too activating” on methyl). Pro tip: Start low and titrate. If overstimulation occurs on methylcobalamin, step down dose, switch to hydroxocobalamin, and ensure hydration/electrolytes.
- Adenosylcobalamin: Great partner for mitochondrial support (often orally combined with methyl).
- Pairing with folate: Use L-methylfolate (5-MTHF) (not folic acid) when supporting methylation. Titrate slowly if sensitive.
- Pairing with folate: Use L-methylfolate (5-MTHF) (not folic acid) when supporting methylation. Titrate slowly if sensitive.
A Little More about the MTHFR Gene Mutation…
*We have a whole different blog on this you can read here:
*The MTHFR gene mutation is very common in the general population. The exact prevalence depends on which variant is being measured:
- C677T mutation
- About 30–40% of the U.S. population carries at least one copy (heterozygous).
Around 10–15% are homozygous (two copies), which has the strongest effect on enzyme activity.
- About 30–40% of the U.S. population carries at least one copy (heterozygous).
- A1298C mutation
- Roughly 30–40% of people carry at least one copy.
- Homozygosity is less clinically impactful than C677T, but still influences folate metabolism.
- Combined mutations (compound heterozygous: C677T + A1298C)
About 10–15% of people carry one of each, which can also impair enzyme function.
Simple Key Points:
- About 40–60% of the general population has some form of MTHFR variant (heterozygous or homozygous).
- Only a smaller subset (10–15%) has variants that significantly reduce enzyme activity and may affect folate/B12 metabolism.
Understanding the four forms of vitamin B12 helps patients make informed decisions about supplementation and treatment. At Nervana Medical in Sandy, Utah, we prioritize the most bioavailable and clinically effective forms, like methylcobalamin and hydroxocobalamin, while also recognizing when adenosylcobalamin or cyanocobalamin may play a role. If you struggle with fatigue, low energy, mood changes, or concerns about MTHFR gene mutations, our team can help tailor a personalized B12 plan to optimize your levels safely and effectively. Book your consultation today at Nervana Medical and discover how the right form of vitamin B12 can support your health, energy, and long-term wellness. *We typically rotate vitamin replacement/optimization for our regular IV/IM patients to ensure best optimization across the board.