Hair loss treatment has changed more in the last five years than in the previous twenty. The studies people quote from 2010 are no longer the studies that should be guiding decisions in 2026. At Nervana Medical in Sandy, UT, our hair loss treatment approach is built around the peer-reviewed literature as it stands today — what’s well-proven, what’s promising, and where we owe patients honesty about the limits.
This post walks through the therapies we use, grouped by how strong the evidence behind each one is. It’s written to be useful to two readers at once: the patient deciding whether to start treatment, and the provider auditing whether our protocol matches the data. If you want the full citation list, our hair restoration service page has the references.
Start with the medical foundation
The most-studied therapies for androgenetic alopecia are still the medical ones. They’re the foundation any plan should be built on, regardless of what biologics or devices get added later.
Topical minoxidil has decades of randomized trial data behind it. It improves scalp blood flow, prolongs the active growth phase of the hair cycle, and produces dose-dependent gains in density. Onset is around 8–12 weeks; maximum effect arrives between months 4 and 6. The first month often involves a synchronized shedding phase, that’s the medication working, not failing.
Low-dose oral minoxidil (typically 1–5 mg for men, 0.5–1 mg for women) has rapidly become a first-line option. A 2025 meta-analysis of nearly 3,000 patients in Frontiers in Pharmacology found efficacy comparable to topical minoxidil with favorable tolerability and a treatment discontinuation rate under 3%. A 2024 JAMA Dermatology head-to-head RCT (Vañó-Galván et al.) found 5 mg once daily non-inferior to topical 5% twice daily in men. We screen blood pressure and cardiac history before starting it.
Topical finasteride is the newer formulation of an old DHT-blocker. A 2024 Journal of Cosmetic Dermatology trial showed topical minoxidil plus topical finasteride 2.2 mg/mL outperformed either monotherapy in men. Systemic absorption is meaningfully lower than the oral pill, which lowers, but doesn’t eliminate, the side-effect profile.
Oral finasteride and dutasteride are the DHT-blockers with the longest track record in men. Head-to-head meta-analysis shows dutasteride 0.5 mg/day produces greater total hair count gains than finasteride 1 mg/day at 24 weeks, with comparable adverse-event rates. We have an honest conversation about sexual side effects (1–4% in pooled trials, usually reversible on discontinuation) before either is prescribed.
Spironolactone is our anti-androgen of choice for premenopausal women with female-pattern loss. A 2023 systematic review found an overall response rate of 56.6%, and the combination of spironolactone plus minoxidil yielded 65.8% improvement versus 43.2% for monotherapy.
Regenerative biologics: where the evidence is moving fast
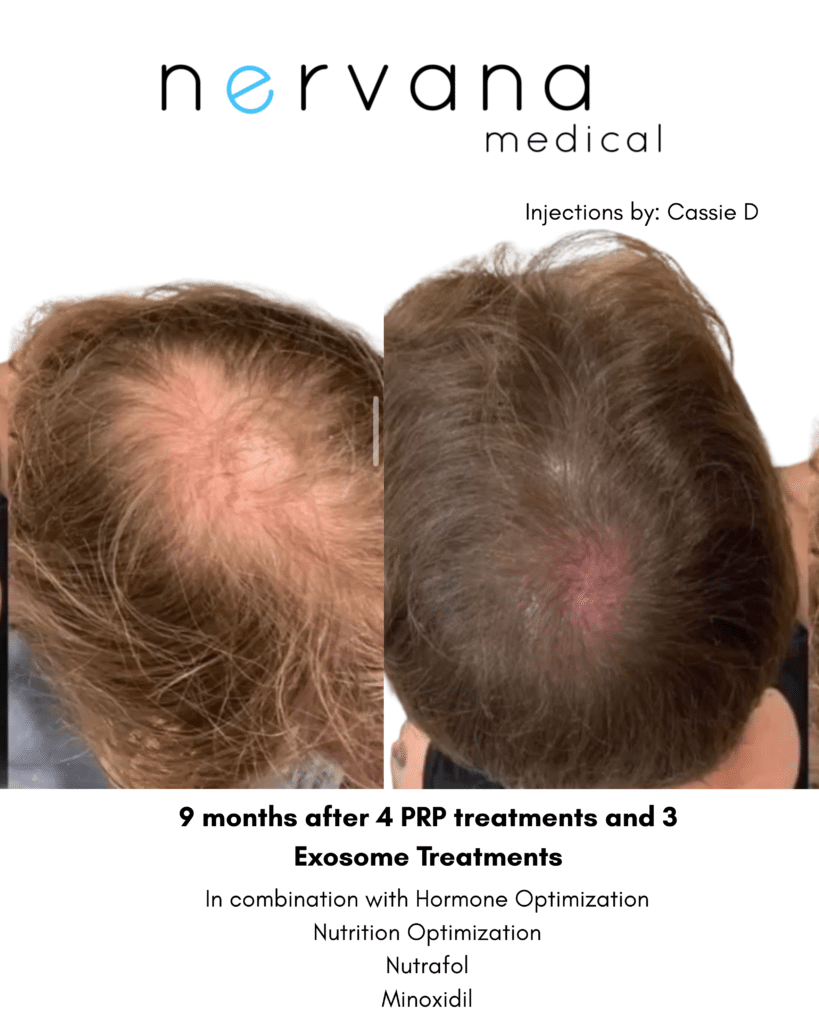
Platelet-rich plasma (PRP) is the most-studied regenerative therapy for hair loss, we’ve written a longer breakdown of PRP, PRF, exosomes, and growth factors for hair restoration for readers who want the mechanism in detail. The short version: your own platelets are concentrated and injected into the scalp, where they release growth factors that wake dormant follicles, thicken existing hairs, and improve scalp health. A 2024 systematic review of 23 RCTs and a 2025 Dermatology and Therapy meta-analysis both confirm statistically significant density gains over placebo at 3 and 6 months.
PRP works best in mild-to-moderate androgenetic alopecia. A prospective study of 93 patients found the strongest responses in Norwood-Hamilton Grade II–III men and Ludwig Grade I women, and a retrospective cohort confirmed response rates of 52% in mild AGA versus only 16% in severe AGA. Younger patients respond better. We’re honest about this: PRP isn’t a rescue for advanced loss.
Platelet-rich fibrin (PRF) is PRP’s next-generation cousin. The same blood draw is processed without anticoagulants, so it forms a fibrin matrix that releases growth factors slowly over 7–14 days. We use it alone, or paired with PRP in a combination protocol designed to give an immediate growth-factor surge alongside sustained release.
Exosomes are nano-sized cellular messengers we deliver topically with microneedling, no blood draw required. A 2025 systematic review in Clinical, Cosmetic and Investigational Dermatology examined 11 clinical studies and reported density gains of 9.5–35 hairs/cm² with a strong safety profile across all sources. The evidence base is smaller and newer than PRP’s, and we say so. Promising, not proven to the same depth.
Adjunctive therapies that pull the foundation forward
Microneedling opens controlled microchannels in the scalp, which improve absorption of topical actives and trigger a wound-healing response that stimulates follicles directly. A 2024 meta-analysis of 12 RCTs found microneedling plus minoxidil produced significantly greater hair count gains than minoxidil alone, with visible response arriving roughly 4 weeks earlier. A 2025 network meta-analysis ranked the combination first among 20 treatment combinations for female AGA.
Low-level light therapy (LLLT) uses red light to stimulate the scalp, painless, no downtime, FDA-cleared. A 2024 meta-analysis of 38 studies (n = 3,098) found significant density gains versus placebo, with the largest effect after 20 weeks of consistent use. Adherence is the variable that matters most.
Why stacking matters
No single therapy is the answer for hair loss. The strongest real-world results come from combining treatments that work at different points in the hair growth cycle, DHT blockade, circulation support, regenerative biologics, and microneedling for absorption. A 2020 meta-analysis of 15 RCTs (1,172 patients) confirmed that minoxidil plus finasteride, minoxidil plus LLLT, and minoxidil plus microneedling were all superior to minoxidil monotherapy.
A 2025 Frontiers in Medicine network meta-analysis ranked PRP + bFGF + minoxidil first among 20 combinations for overall efficacy. Combination therapy isn’t a marketing concept, it’s where the data points.
We can’t miss the whole picture of health
This is where being an integrative practice matters. Before we start any plan, we look at what’s actually driving the loss. That means screening ferritin, vitamin D, B12, and thyroid; reviewing hormones (especially in perimenopause); asking about stress, sleep, and the medications people are on. A patient with low ferritin and untreated thyroid disease will not respond well to PRP, no matter how good the protocol is.
Nervana Medical is built around this idea. Aesthetic injectables sit alongside hormone replacement therapy, IV and NAD+ therapy, iron replacement and mental health care under one roof, so a hair-loss consult naturally extends into the upstream questions that often matter most. It’s the part of hair restoration that gets skipped in injection-only clinics and it’s the part that determines whether the rest of the plan actually works.
How we keep ourselves honest
We re-photograph at 3 and 6 months using a standardized scalp camera position, and we review the images with you. Trichoscopy lets us track hair diameter variability and the vellus-to-terminal ratio, the same endpoints used in the published literature. If a treatment isn’t working at 6 months, we say so and change the plan. Hair restoration isn’t a sales pitch. It’s a series of evidence-based decisions reviewed on a real timeline.
Frequently Asked Questions
How long before I see results from hair loss treatment?
Most pharmacologic therapies need a minimum of 3–6 months before meaningful changes are detectable, with maximum benefit often arriving between 12 and 24 months. PRP series typically show density and thickness gains at the 3- and 6-month re-imaging visits. Anyone promising results in a few weeks is overselling.
Is PRP better than minoxidil?
Head-to-head, no; a 2026 meta-analysis of 9 RCTs found no significant difference in hair density between PRP and topical minoxidil alone. The combination of PRP plus minoxidil consistently outperforms either monotherapy, which is why we stack them rather than choose between them.
Who is the best candidate for PRP?
The strongest responders are patients with mild-to-moderate androgenetic alopecia, younger age, and treatment-naïve or partial-response status. PRP is not a rescue therapy for advanced loss , by the time follicles are terminally miniaturized, there are fewer targets for growth-factor stimulation.
Are oral minoxidil and finasteride safe?
In published trials, both have favorable safety profiles when dosed appropriately and screened for the right patient. Low-dose oral minoxidil has a discontinuation rate under 3% in pooled data; finasteride has a 1–4% rate of sexual side effects that are usually reversible. We screen blood pressure and cardiac history before oral minoxidil, and we have a real conversation about DHT-blocker side effects before any prescription.
Do I have to do this forever?
Hair-loss treatment for androgenetic alopecia is maintenance, not cure. Stopping minoxidil reliably returns hair to baseline within 4–6 months. PRP requires periodic boosters every 3–6 months to sustain results. We’re upfront about this at the consult so the plan you start is one you’re prepared to stay on.
Book a Hair Restoration Consultation in Sandy, UT
A real plan starts with a real assessment ; your pattern, your bloodwork, your goals, and an honest conversation about what the evidence supports. If you’re thinking about treatment, book a consultation and let’s look at the whole picture together.